Fall 2022 SOWK 486w Week 09 - Lab Day - Assessments
A presentation at Heritage University @ CBC Week 09 in in Pasco, WA 99301, USA by Jacob Campbell
Assessments Lab Day gathering information and formulating it into a coherent picture of the client and his or her circumstances Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486
Social histories Agenda Implicit Bias Teach Back Activity Genograms & Eco-maps Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Examples of Writing Resilience and Dimensions of APA Style Website My Feedback Applied Transdisciplinarity Example Papers Document Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486
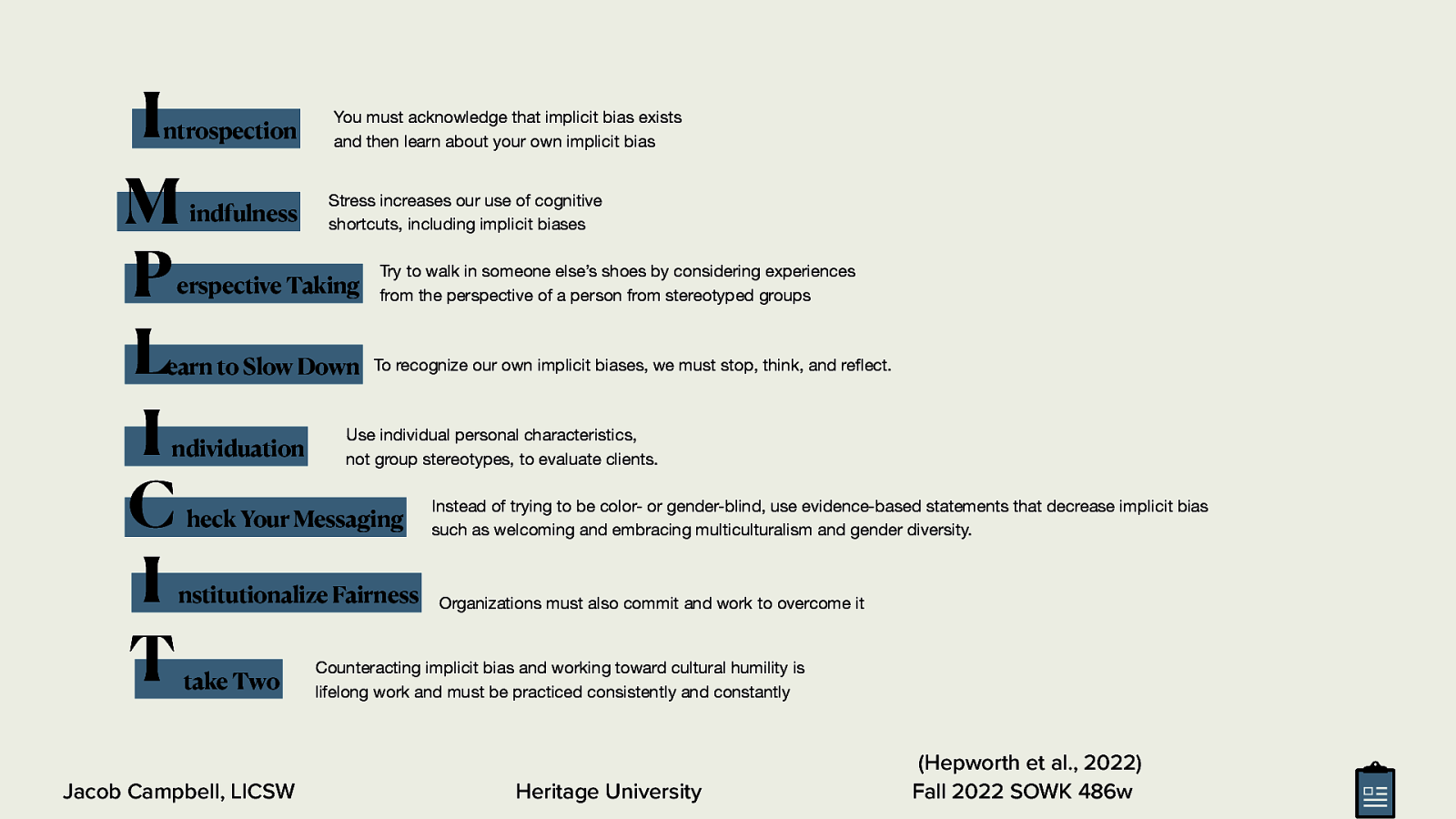
I M P L I C I T ntrospection indfulness You must acknowledge that implicit bias exists and then learn about your own implicit bias Stress increases our use of cognitive shortcuts, including implicit biases erspective Taking earn to Slow Down ndividuation Try to walk in someone else’s shoes by considering experiences from the perspective of a person from stereotyped groups To recognize our own implicit biases, we must stop, think, and re ect. Use individual personal characteristics, not group stereotypes, to evaluate clients. heck Your Messaging nstitutionalize Fairness take Two Instead of trying to be color- or gender-blind, use evidence-based statements that decrease implicit bias such as welcoming and embracing multiculturalism and gender diversity. Organizations must also commit and work to overcome it Counteracting implicit bias and working toward cultural humility is lifelong work and must be practiced consistently and constantly Heritage University fl Jacob Campbell, LICSW (Hepworth et al., 2022) Fall 2022 SOWK 486w
https://implicit.harvard.edu/implicit/selectatest.html Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem Life Experiences Impressions and Recommendations Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem Impressions and Recommendations • Description and history of the presenting problem • Introductory section Life Experiences Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem • Description and history of the presenting problem • Introductory section Impressions and Recommendations • Presenting problem Detail major points Generally the “why are you here today section” Life Experiences Jacob Campbell, LICSW My method for mental health evaluations Heritage University Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem Esmeralda, a 32 year old Hispanic married with three children female completed this mental health evaluation at the TCCH BHS Pasco o ce. She was accompanied by her husband and one child. Her primary language is Spanish, and the evaluation was completed in her native language. Her insurance, Medicaid, has been veri ed. She was referred by Crisis Response Unit after being hospitalized at Lourdes Medical Center after an attempted suicide. She presented with symptoms related to depression and anxiety. Impressions and Recommendations Life Experiences Heritage University fi ffi Jacob Campbell, LICSW Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem • Family of origin • Birth and childhood Impressions and Recommendations • Marriages and signi cant relationships • Current living arrangements • Education Life Experiences fi Jacob Campbell, LICSW • Military service Heritage University Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem • Employment history • Medical history Impressions and Recommendations • Legal history • Social and recreational interests • Religious activities Life Experiences Jacob Campbell, LICSW • Client successes, strengths, and resources Heritage University Fall 2022 SOWK 486w
Layout of the Social History Presenting Problem Impressions and Recommendations • Impressions • Recommendations Life Experiences Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
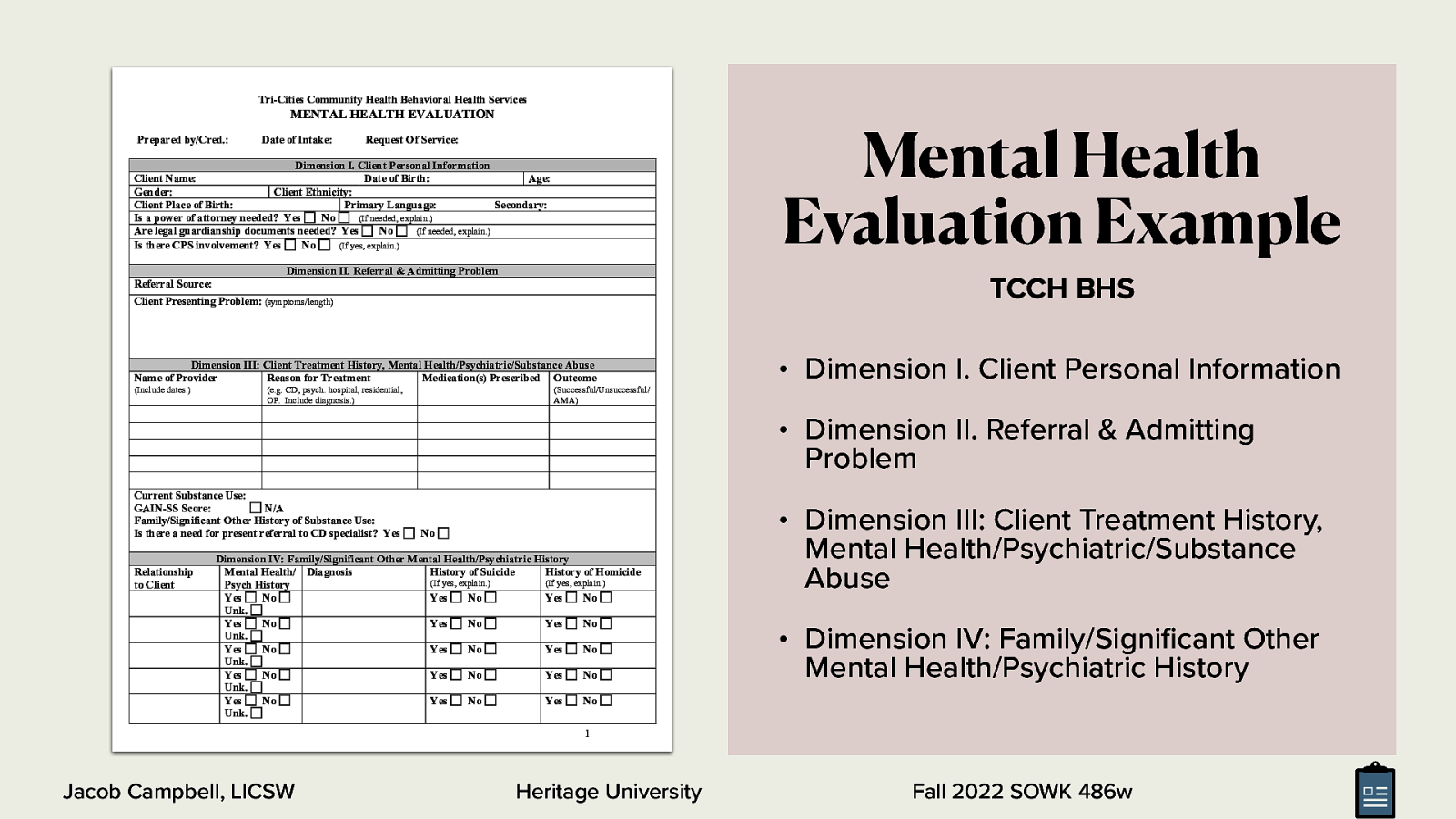
Tri-Cities Community Health Behavioral Health Services Mental Health Evaluation Example MENTAL HEALTH EVALUATION Prepared by/Cred.: Date of Intake: Request Of Service: Dimension I. Client Personal Information Client Name: Date of Birth: Age: Gender: Client Ethnicity: Client Place of Birth: Primary Language: Secondary: Is a power of attorney needed? Yes No (If needed, explain.) Are legal guardianship documents needed? Yes No (If needed, explain.) Is there CPS involvement? Yes No (If yes, explain.) Dimension II. Referral & Admitting Problem TCCH BHS Referral Source: Client Presenting Problem: (symptoms/length) Dimension III: Client Treatment History, Mental Health/Psychiatric/Substance Abuse Name of Provider Reason for Treatment Medication(s) Prescribed Outcome (Include dates.) (e.g. CD, psych. hospital, residential, OP. Include diagnosis.) • Dimension I. Client Personal Information (Successful/Unsuccessful/ AMA) • Dimension II. Referral & Admitting Problem Current Substance Use: GAIN-SS Score: N/A Family/Significant Other History of Substance Use: Is there a need for present referral to CD specialist? Yes Relationship to Client No Dimension IV: Family/Significant Other Mental Health/Psychiatric History Mental Health/ Diagnosis History of Suicide History of Homicide (If yes, explain.) (If yes, explain.) Psych History Yes No Yes No Yes No Unk. Yes No Yes No Yes No Unk. Yes No Yes No Yes No Unk. Yes No Yes No Yes No Unk. Yes No Yes No Yes No Unk. • Dimension III: Client Treatment History, Mental Health/Psychiatric/Substance Abuse • Dimension IV: Family/Signi cant Other Mental Health/Psychiatric History 1 Heritage University fi Jacob Campbell, LICSW Fall 2022 SOWK 486w
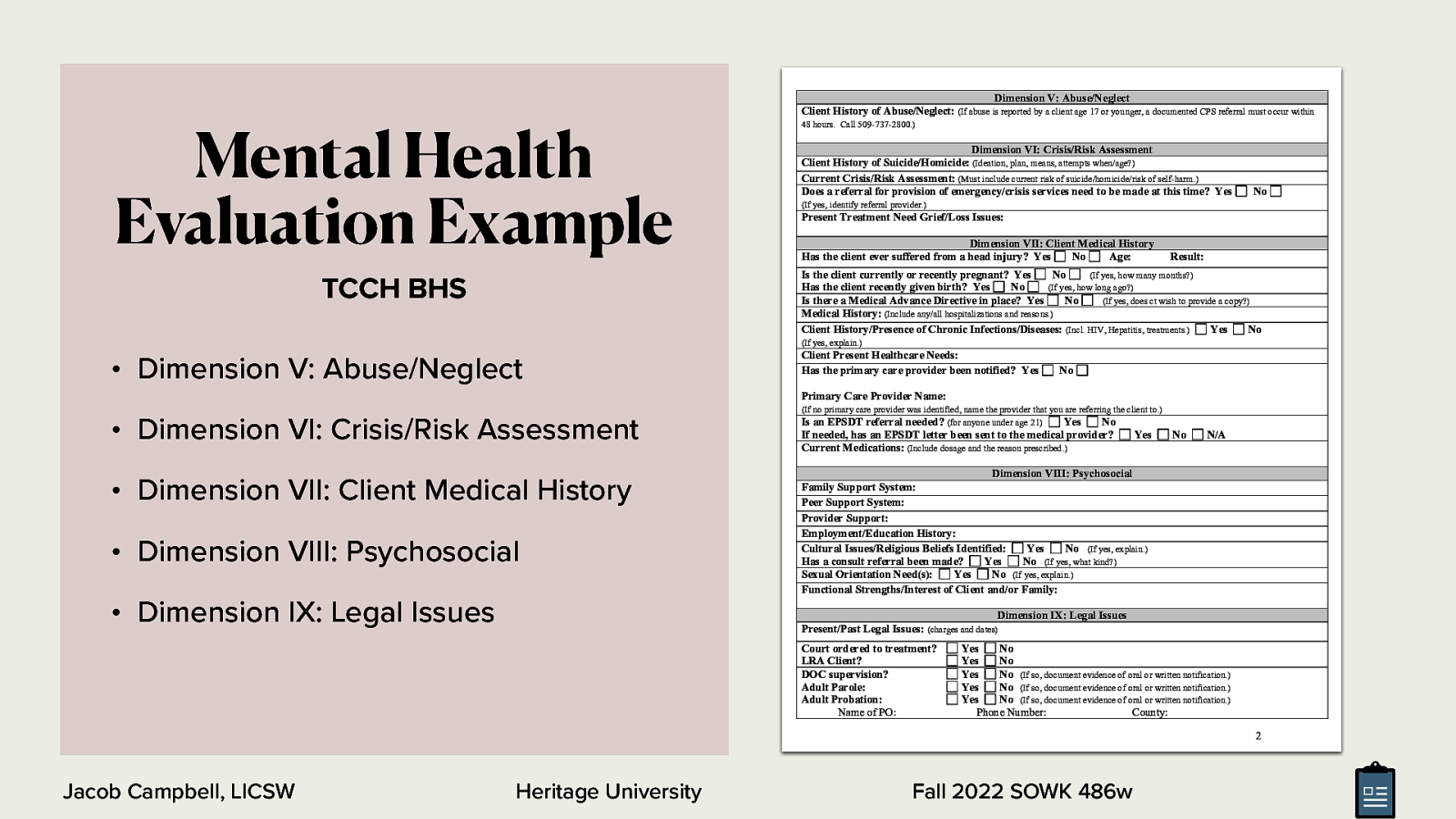
Mental Health Evaluation Example Dimension V: Abuse/Neglect Client History of Abuse/Neglect: (If abuse is reported by a client age 17 or younger, a documented CPS referral must occur within 48 hours. Call 509-737-2800.) Dimension VI: Crisis/Risk Assessment Client History of Suicide/Homicide: (Ideation, plan, means, attempts when/age?) Current Crisis/Risk Assessment: (Must include current risk of suicide/homicide/risk of self-harm.) Does a referral for provision of emergency/crisis services need to be made at this time? Yes No (If yes, identify referral provider.) Present Treatment Need Grief/Loss Issues: Dimension VII: Client Medical History Has the client ever suffered from a head injury? Yes No Age: Result: Is the client currently or recently pregnant? Yes No (If yes, how many months?) Has the client recently given birth? Yes No (If yes, how long ago?) Is there a Medical Advance Directive in place? Yes No (If yes, does ct wish to provide a copy?) Medical History: (Include any/all hospitalizations and reasons.) Client History/Presence of Chronic Infections/Diseases: (Incl. HIV, Hepatitis, treatments.) Yes No TCCH BHS (If yes, explain.) • Dimension V: Abuse/Neglect Client Present Healthcare Needs: Has the primary care provider been notified? Yes No Primary Care Provider Name: • Dimension VI: Crisis/Risk Assessment • Dimension VII: Client Medical History • Dimension VIII: Psychosocial • Dimension IX: Legal Issues (If no primary care provider was identified, name the provider that you are referring the client to.) Is an EPSDT referral needed? (for anyone under age 21) Yes No If needed, has an EPSDT letter been sent to the medical provider? Current Medications: (Include dosage and the reason prescribed.) Yes No N/A Dimension VIII: Psychosocial Family Support System: Peer Support System: Provider Support: Employment/Education History: Cultural Issues/Religious Beliefs Identified: Yes No (If yes, explain.) Has a consult referral been made? Yes No (If yes, what kind?) Sexual Orientation Need(s): Yes No (If yes, explain.) Functional Strengths/Interest of Client and/or Family: Dimension IX: Legal Issues Present/Past Legal Issues: (charges and dates) Court ordered to treatment? LRA Client? DOC supervision? Adult Parole: Adult Probation: Name of PO: Yes No Yes No Yes No (If so, document evidence of oral or written notification.) Yes No (If so, document evidence of oral or written notification.) Yes No (If so, document evidence of oral or written notification.) Phone Number: County: 2 Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
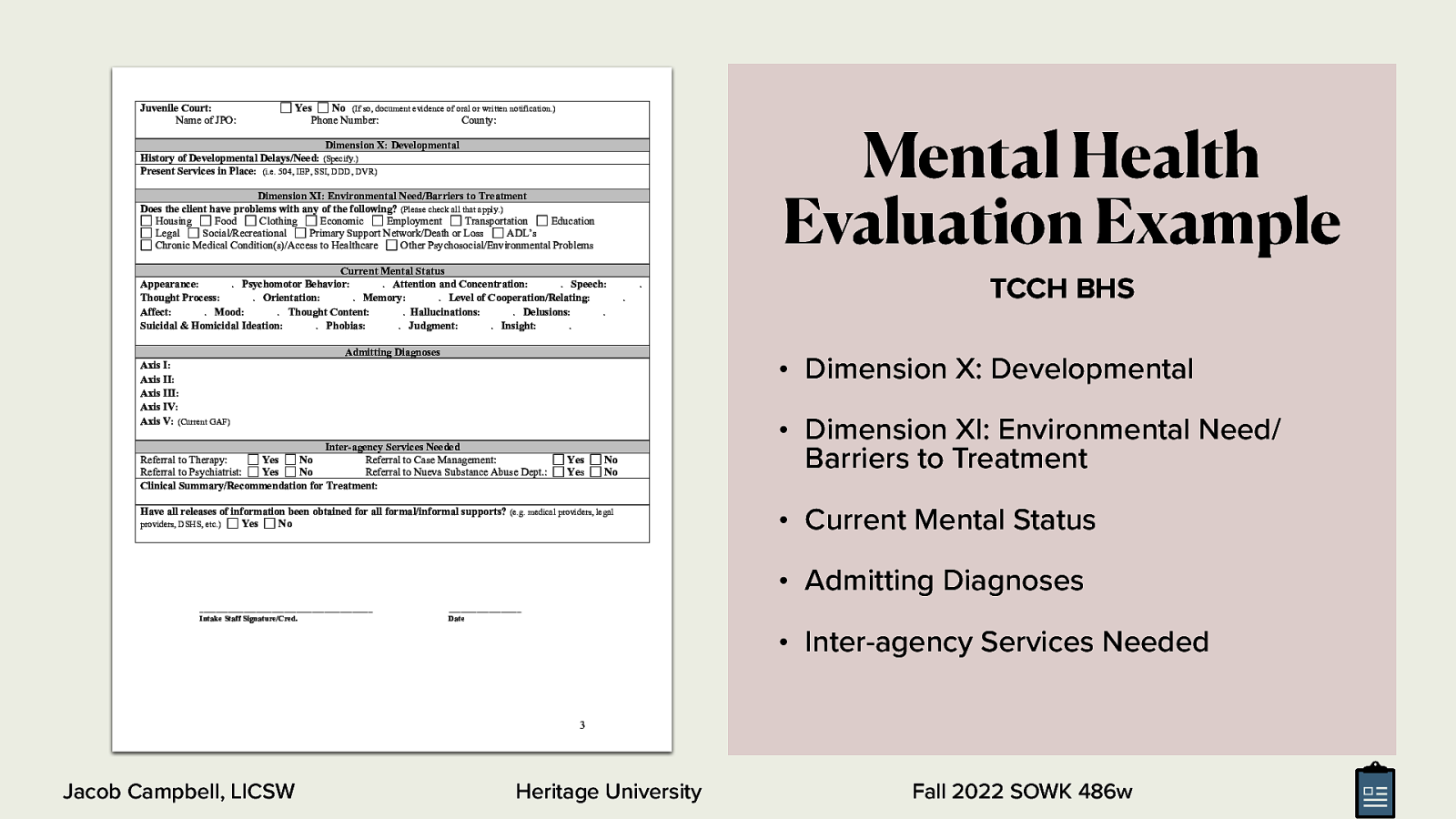
Juvenile Court: Name of JPO: Yes No (If so, document evidence of oral or written notification.) Phone Number: County: Mental Health Evaluation Example Dimension X: Developmental History of Developmental Delays/Need: (Specify.) Present Services in Place: (i.e. 504, IEP, SSI, DDD, DVR) Dimension XI: Environmental Need/Barriers to Treatment Does the client have problems with any of the following? (Please check all that apply.) Housing Food Clothing Economic Employment Transportation Education Legal Social/Recreational Primary Support Network/Death or Loss ADL’s Chronic Medical Condition(s)/Access to Healthcare Other Psychosocial/Environmental Problems Current Mental Status Appearance: . Psychomotor Behavior: . Attention and Concentration: . Speech: Thought Process: . Orientation: . Memory: . Level of Cooperation/Relating: Affect: . Mood: . Thought Content: . Hallucinations: . Delusions: . Suicidal & Homicidal Ideation: . Phobias: . Judgment: . Insight: . . . Admitting Diagnoses TCCH BHS • Dimension X: Developmental Axis I: Axis II: Axis III: Axis IV: Axis V: (Current GAF) Inter-agency Services Needed Referral to Therapy: Yes No Referral to Case Management: Referral to Psychiatrist: Yes No Referral to Nueva Substance Abuse Dept.: Clinical Summary/Recommendation for Treatment: Yes Yes No No Have all releases of information been obtained for all formal/informal supports? (e.g. medical providers, legal providers, DSHS, etc.) Yes No • Dimension XI: Environmental Need/ Barriers to Treatment • Current Mental Status • Admitting Diagnoses ___________________________________________ Intake Staff Signature/Cred. __________________ Date • Inter-agency Services Needed 3 Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Practice with Social Histories • Family of origin • Employment history • Birth and childhood • Medical history • Marriages and signi cant relationships • Legal history • Current living arrangements • Education • Military service fi Jacob Campbell, LICSW • Social and Recreational interests • Religious activities Work with a partner to go through some of the process of completing a social history with them. You can either use real life information or make up informational a part of a role-play. • Client successes, Strengths, and resources Heritage University Fall 2022 SOWK 486w
Students are to develop a 5-10 minute short presentation teaching your peers about assessing the chosen area. • Assessing biophysical Functioning (pp. 168-172) • Assessing Cognitive/Perceptual Functioning (pp. 172-176) This Week • Assessing A ective Functioning (pp. 176-180) • Assessing Behavioral Functioning (pp. 180-182) • Assessing Environmental System (pp. 182-186) Group Discussion (Hepworth et al., 2022) Jacob Campbell, LICSW ff In Class Teach Back Activity Heritage University Fall 2022 SOWK 486 Provide Info

campbell_j@heritage.edu Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Family Assessments Eco-Map A E P Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Mini Mental Status Exams Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Mental Status Exam The General Components • General appearance • Intelligence • Behavior • Reality testing • Thought process and content • Suicidal or homicidal ideation • A ect • Judgment • Impulse control • Insight • Cognitive functioning ff Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
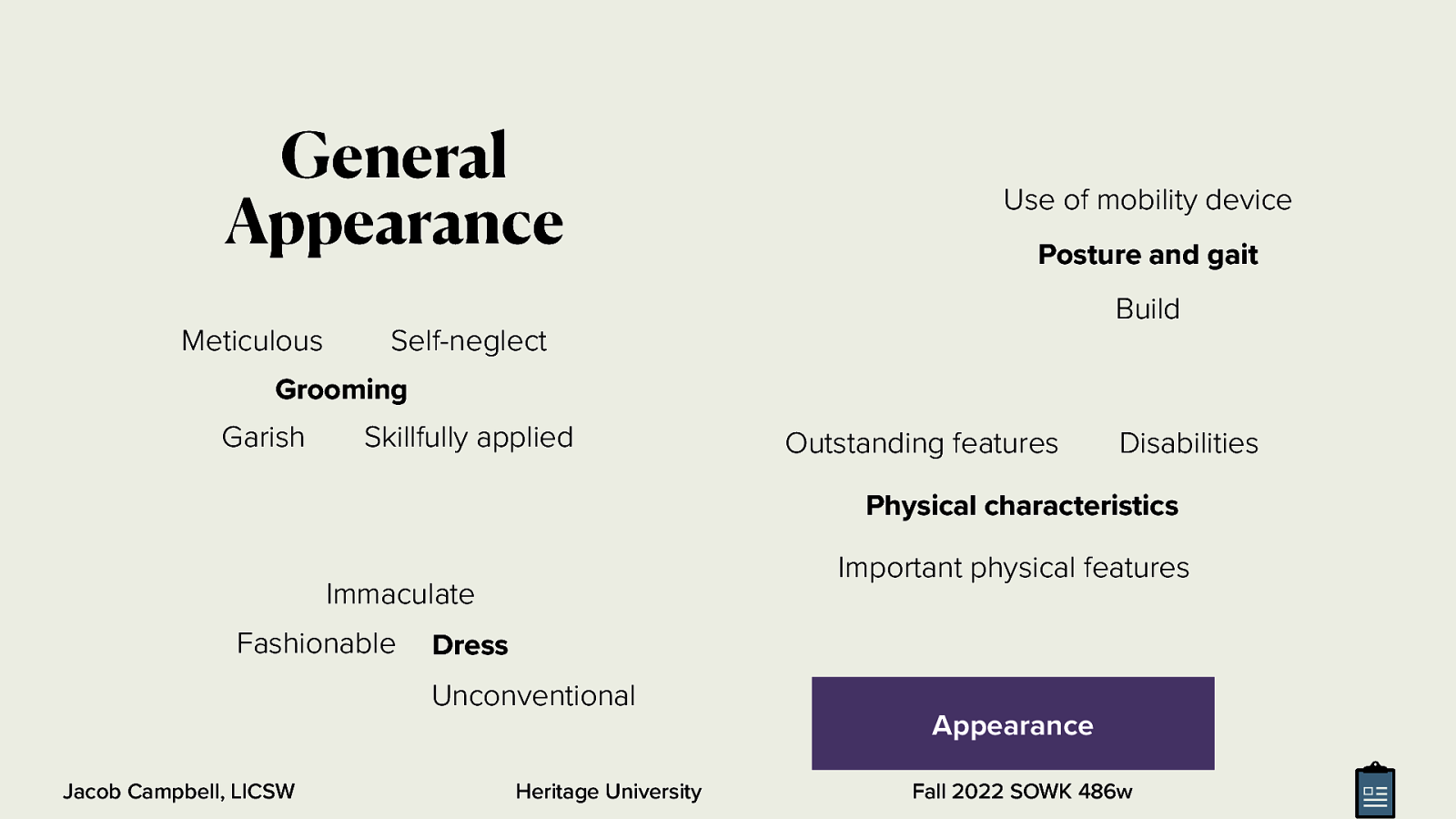
General Appearance Use of mobility device Posture and gait Build Meticulous Self-neglect Grooming Garish Skillfully applied Outstanding features Disabilities Physical characteristics Important physical features Immaculate Fashionable Dress Unconventional Jacob Campbell, LICSW Heritage University Appearance Fall 2022 SOWK 486w

General Appearance Passive Sullen Ingratiating Guarded Hostility Seductive Attitude and Interpersonal Style Uncooperative Demanding Jacob Campbell, LICSW Manipulative Heritage University Playful Inappropriate boundaries Contemptuous Withdrawn Fall 2022 SOWK 486w
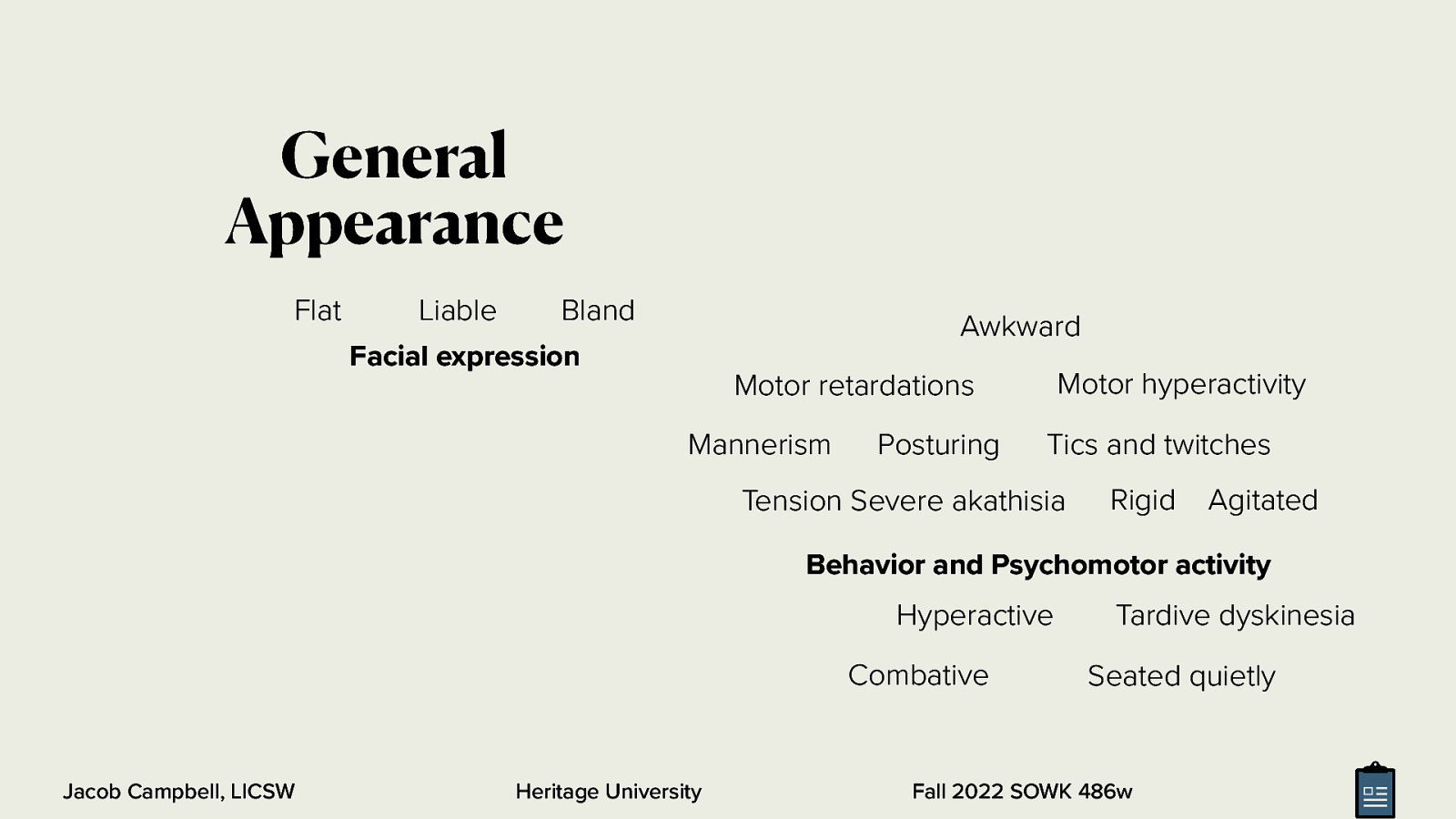
General Appearance Flat Liable Bland Facial expression Awkward Motor hyperactivity Motor retardations Mannerism Posturing Tics and twitches Tension Severe akathisia Rigid Agitated Behavior and Psychomotor activity Hyperactive Combative Jacob Campbell, LICSW Heritage University Tardive dyskinesia Seated quietly Fall 2022 SOWK 486w
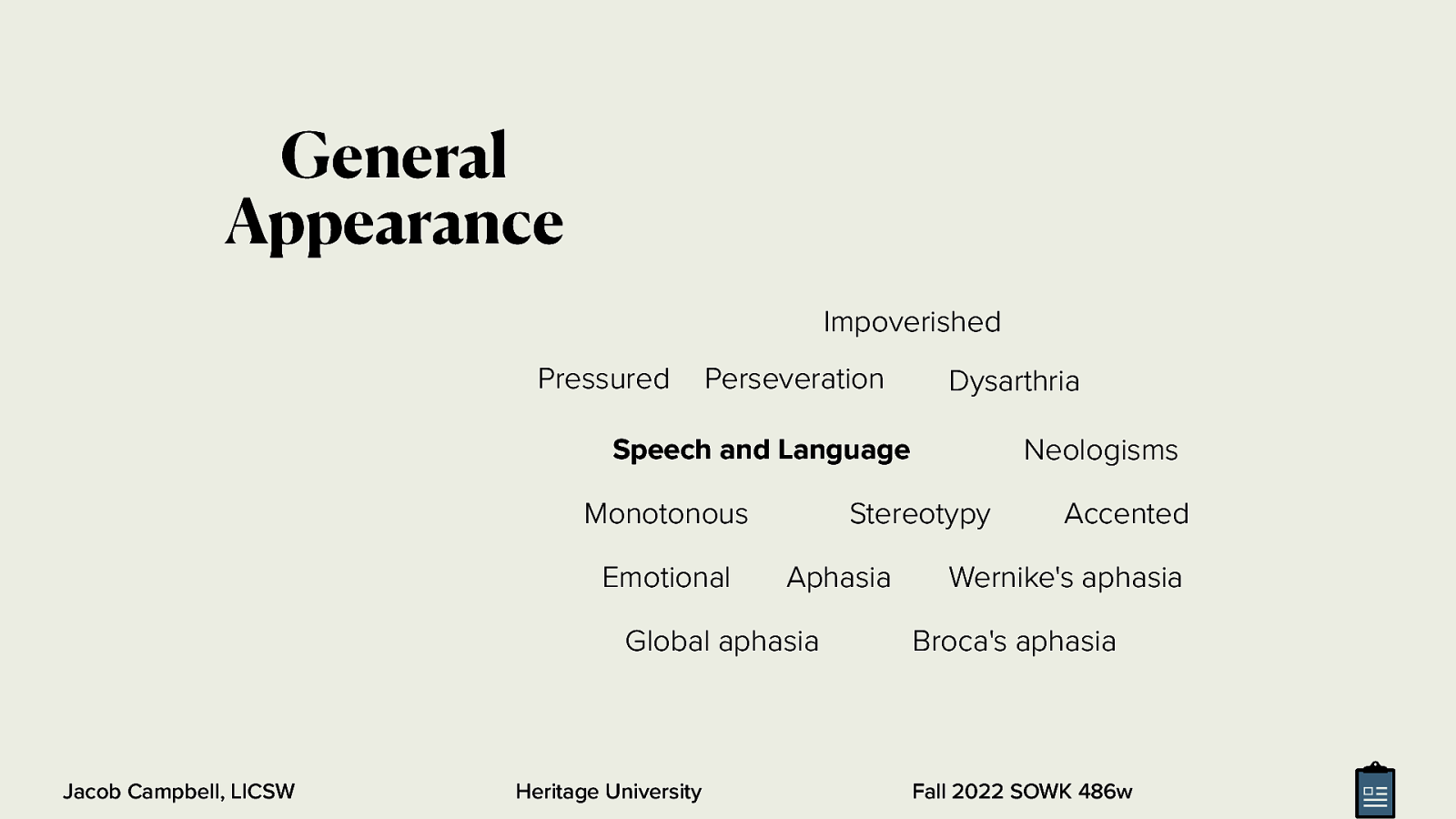
General Appearance Impoverished Pressured Perseveration Dysarthria Neologisms Speech and Language Monotonous Emotional Stereotypy Aphasia Global aphasia Jacob Campbell, LICSW Heritage University Accented Wernike’s aphasia Broca’s aphasia Fall 2022 SOWK 486w
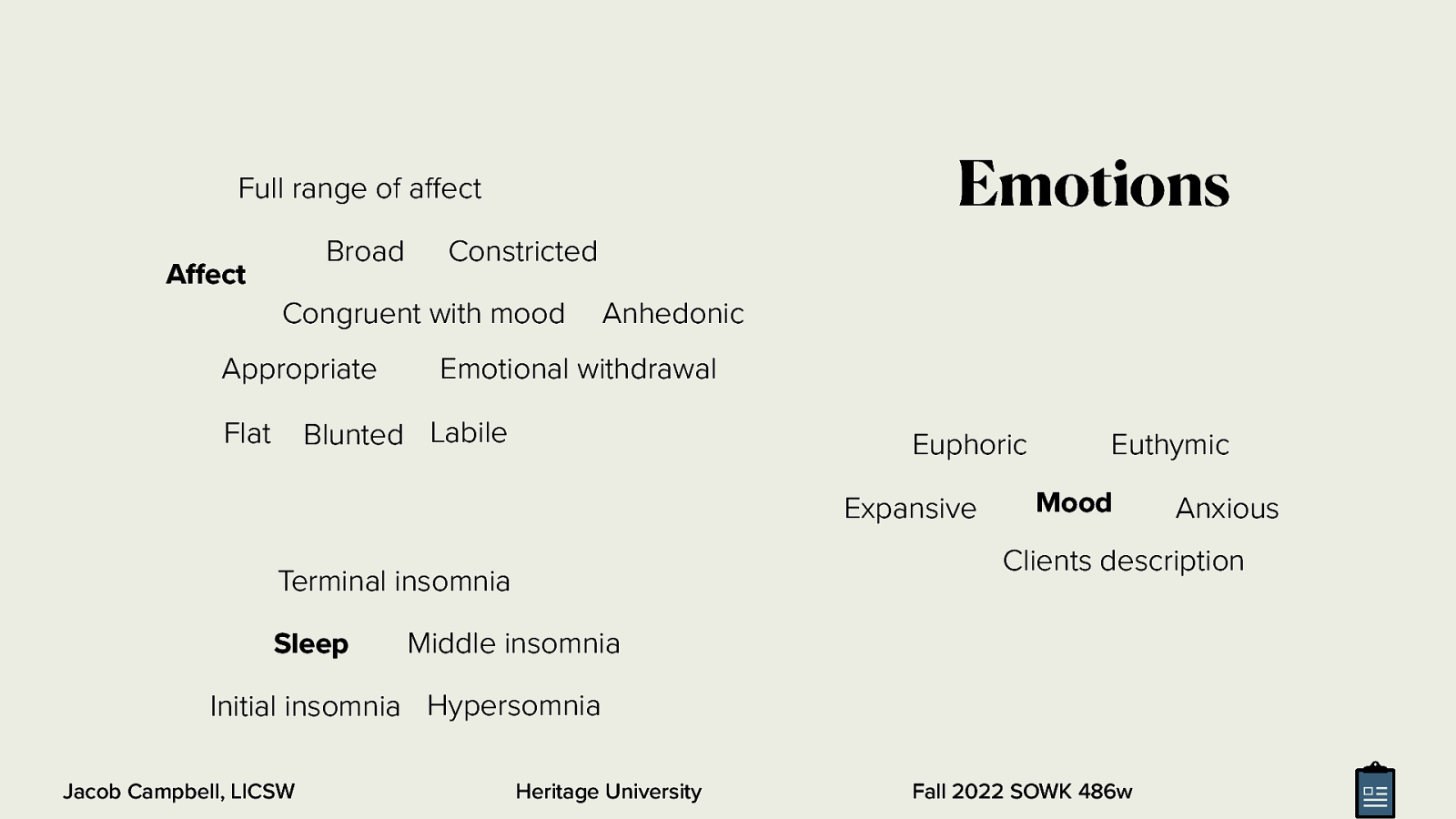
Emotions Full range of a ect Broad A ect Constricted Congruent with mood Appropriate Anhedonic Emotional withdrawal Blunted Labile Flat Euphoric Expansive Mood Middle insomnia Initial insomnia Hypersomnia ff ff Jacob Campbell, LICSW Anxious Clients description Terminal insomnia Sleep Euthymic Heritage University Fall 2022 SOWK 486w
Cognitive Functioning Lethargy Attention and concentration Oriented Times Four Orientation and level of consciousness Coma Stupor Obtundation Anterograde amnesia Transient global amnesia Amnesia Retrograde amnesia Memory Registration Retention Retrieval Short term memory Jacob Campbell, LICSW Heritage University Head Injuries Long term memory Fall 2022 SOWK 486w
Cognitive Functioning Memory Testing Ability to Abstract and Generalize Information Intelligence Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Somatic delusions Nihilistic delusions Thought Content Delusions Bizarre behavior Grandiose delusions Delusional guilt Ideas of inference Thought content Magical thinking Thoughts and Perception Ideas of reference Distortions Though broadcasting Suspiciousness Paranoid delusions Thought withdrawal Thought insertion Illusions Hallucinations Disordered Perceptions Dearealization Jacob Campbell, LICSW Depersonalization Heritage University Fall 2022 SOWK 486w
Thoughts and Perception Loose association Perseverative Racing thoughts Conceptual disorganization Neologism Overvalued Thought Process Distractable Goal directed Spontaneous Incoherent Circumstantial Jacob Campbell, LICSW Heritage University Tangentiality Clang association Illogical Flight of ideas blocking Impoverished Fall 2022 SOWK 486w
Somatic preoccupations Phobias Preoccupations Obsessions Compulsions Suicidality, Homicidality, Impulse control Jacob Campbell, LICSW Heritage University Thoughts and Perception Insight and Judgment Fall 2022 SOWK 486w
The Checklist Manifesto Hot to Get things Done Right Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
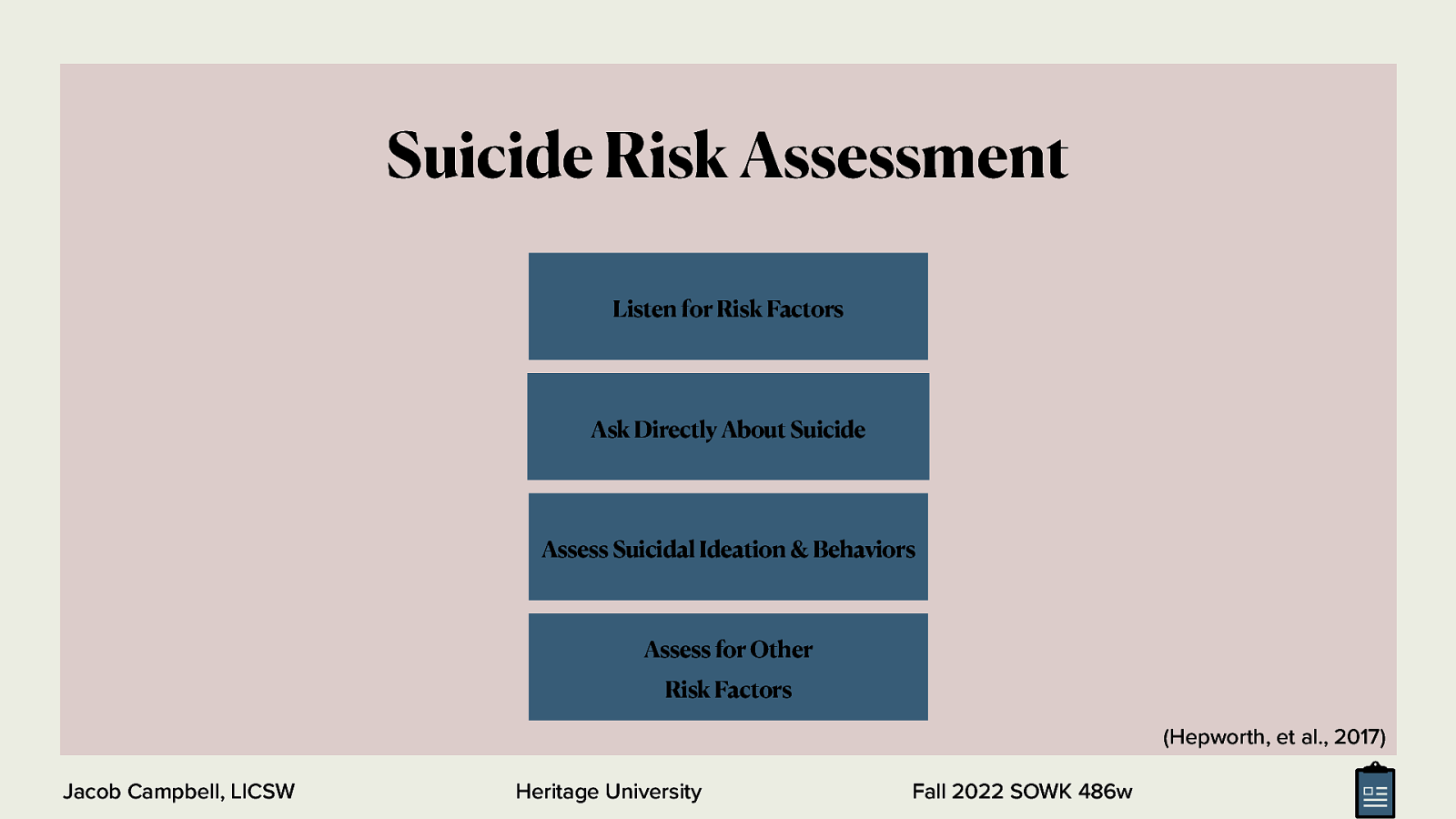
Suicide Risk Assessment Listen for Risk Factors Ask Directly About Suicide Assess Suicidal Ideation & Behaviors Assess for Other Risk Factors (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
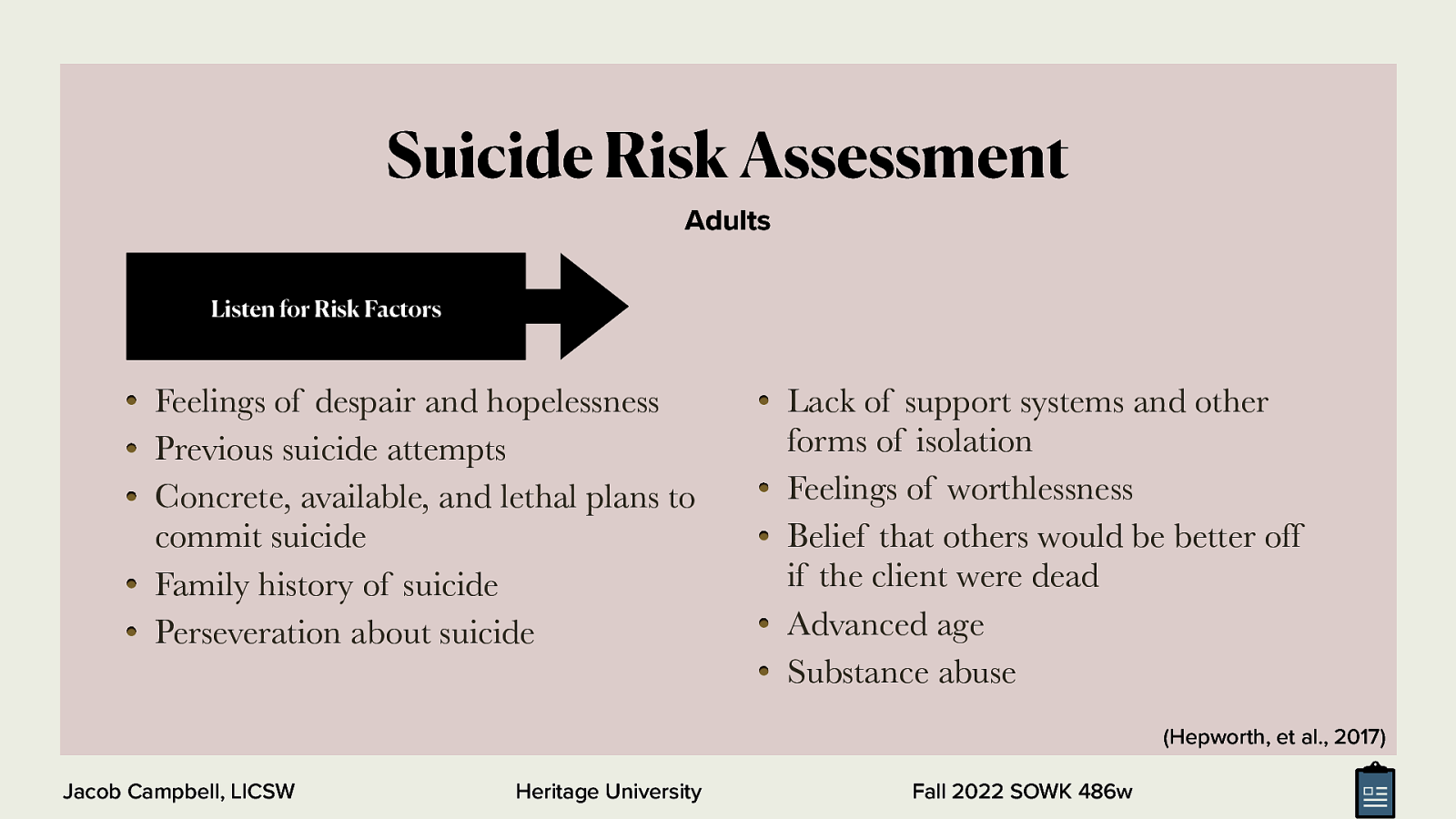
Suicide Risk Assessment Adults Listen for Risk Factors Feelings of despair and hopelessness Previous suicide attempts Concrete, available, and lethal plans to commit suicide Family history of suicide Perseveration about suicide Lack of support systems and other forms of isolation Feelings of worthlessness Belief that others would be better off if the client were dead Advanced age Substance abuse (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
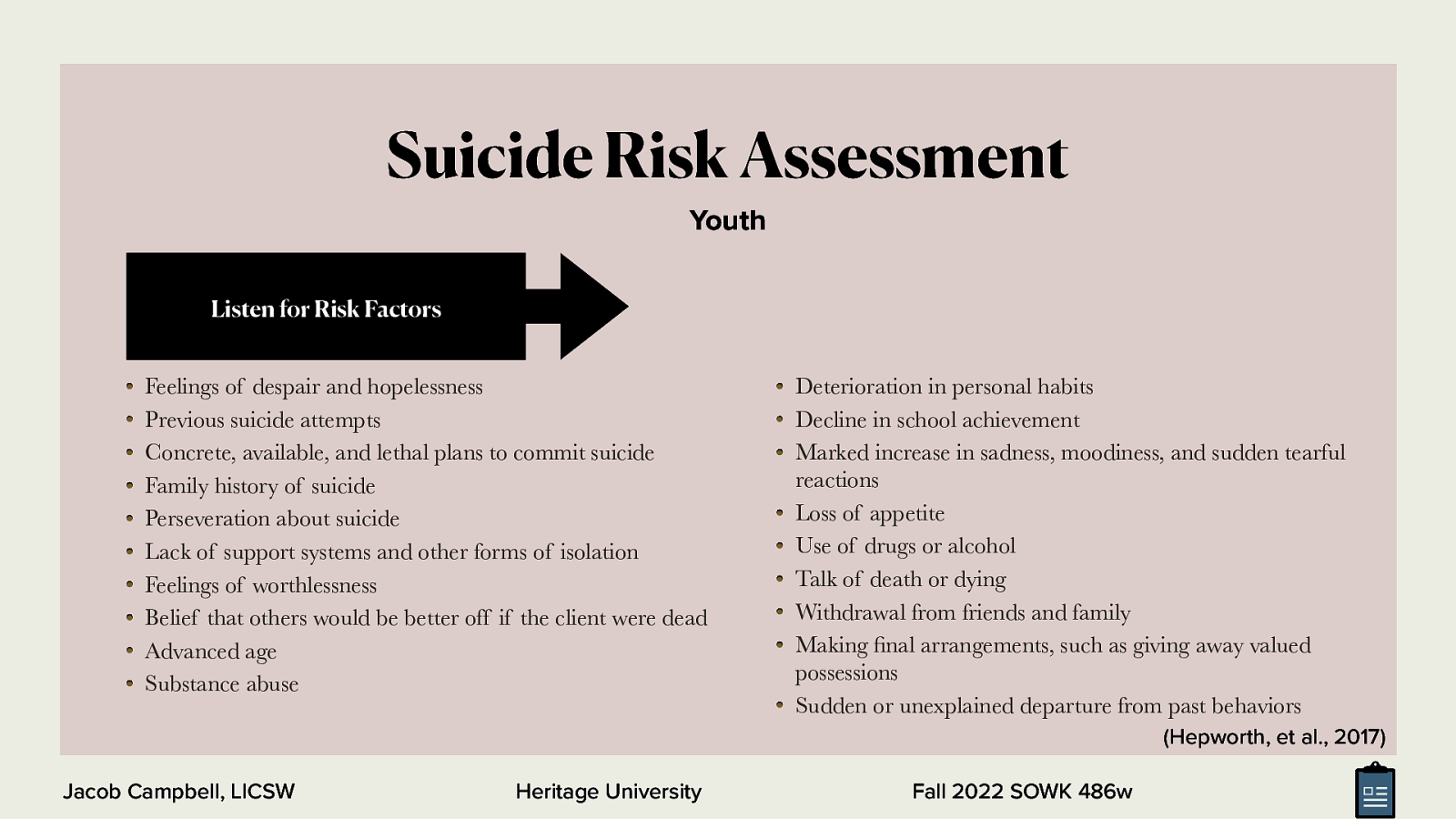
Suicide Risk Assessment Youth Listen for Risk Factors Feelings of despair and hopelessness Previous suicide attempts Concrete, available, and lethal plans to commit suicide Family history of suicide Perseveration about suicide Lack of support systems and other forms of isolation Feelings of worthlessness Belief that others would be better off if the client were dead Advanced age Substance abuse Deterioration in personal habits Decline in school achievement Marked increase in sadness, moodiness, and sudden tearful reactions Loss of appetite Use of drugs or alcohol Talk of death or dying Withdrawal from friends and family Making nal arrangements, such as giving away valued possessions Sudden or unexplained departure from past behaviors (Hepworth, et al., 2017) fi Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
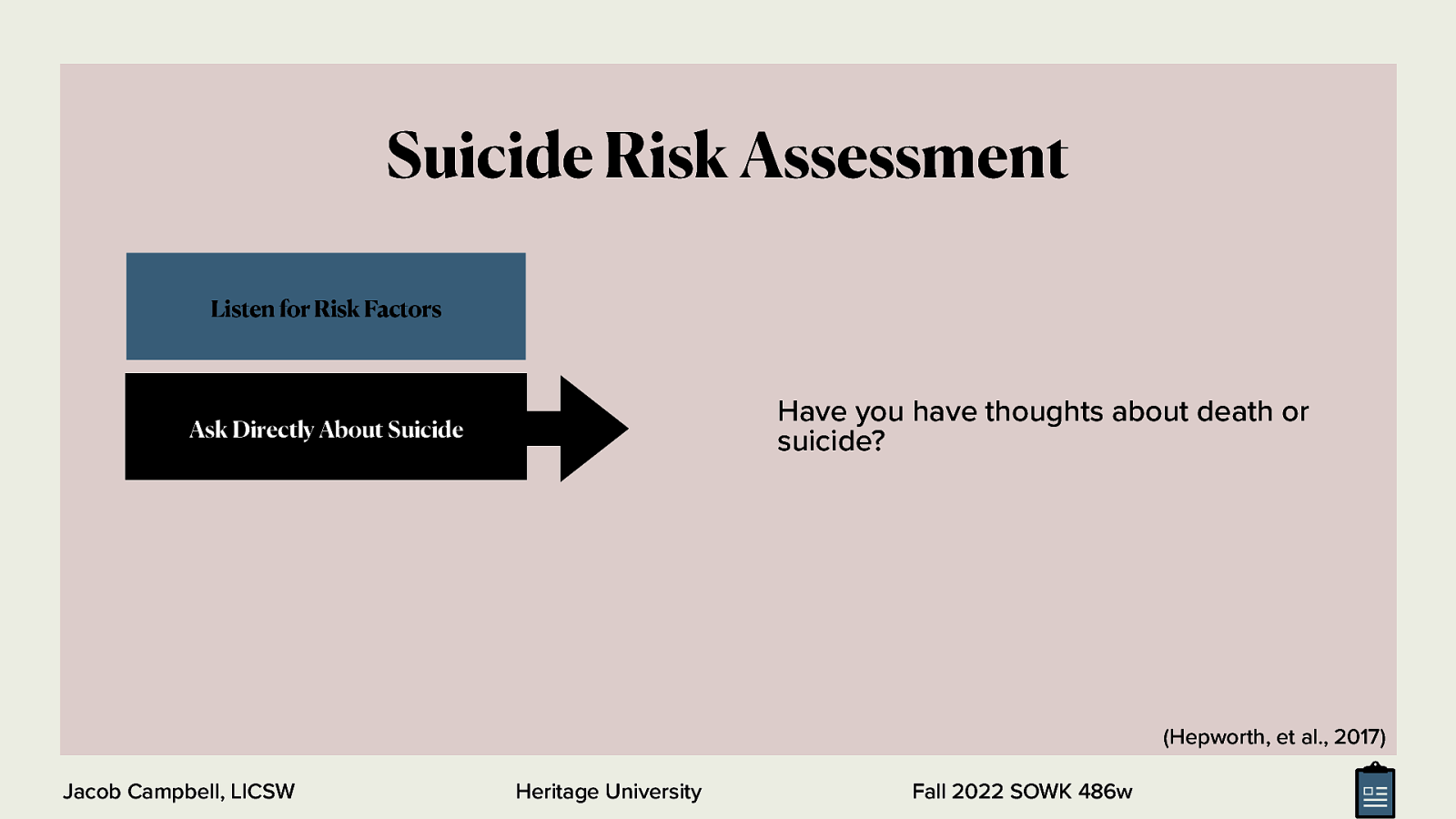
Suicide Risk Assessment Listen for Risk Factors Have you have thoughts about death or suicide? Ask Directly About Suicide (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
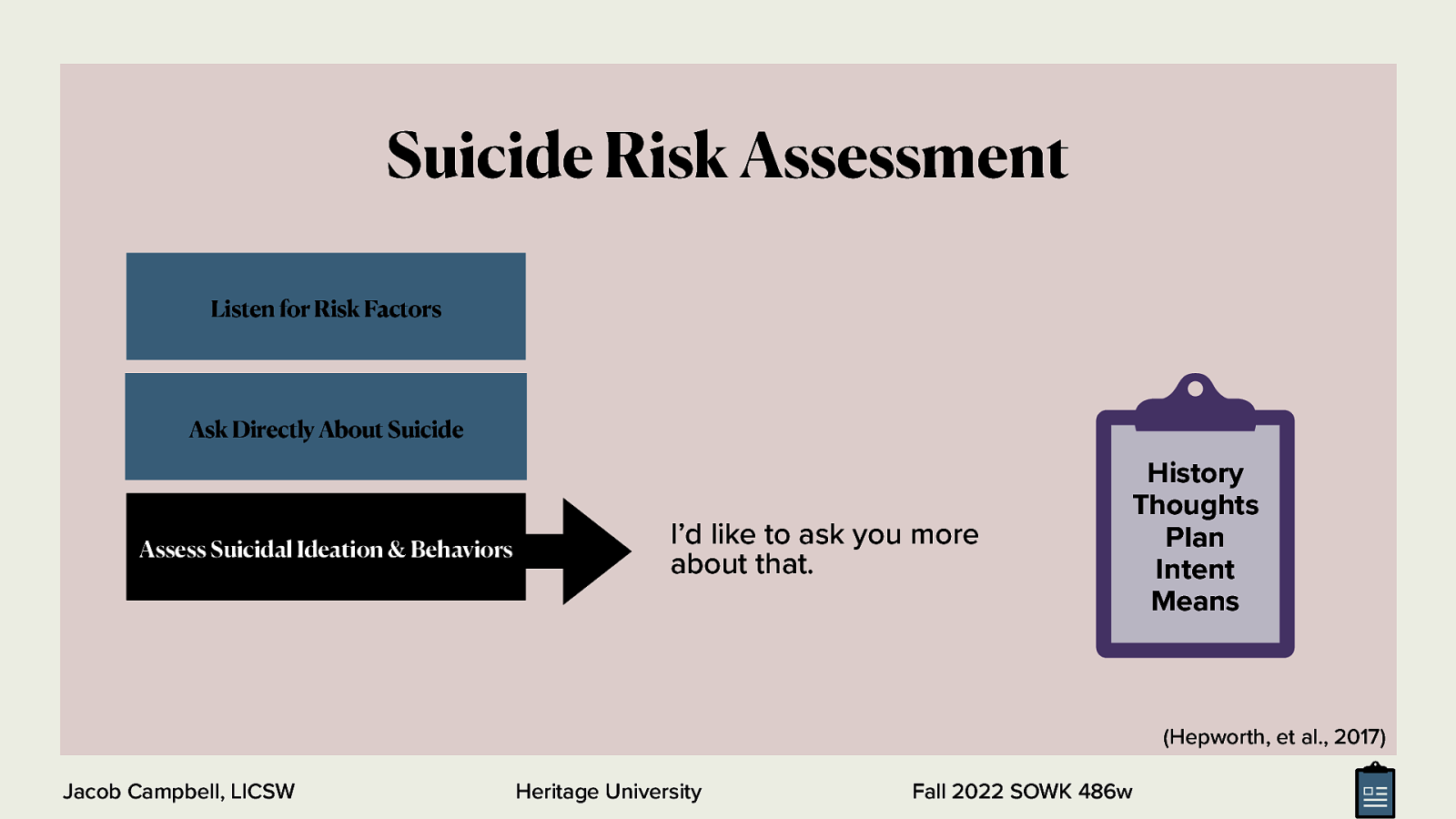
Suicide Risk Assessment Listen for Risk Factors Ask Directly About Suicide Assess Suicidal Ideation & Behaviors I’d like to ask you more about that. History Thoughts Plan Intent Means (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
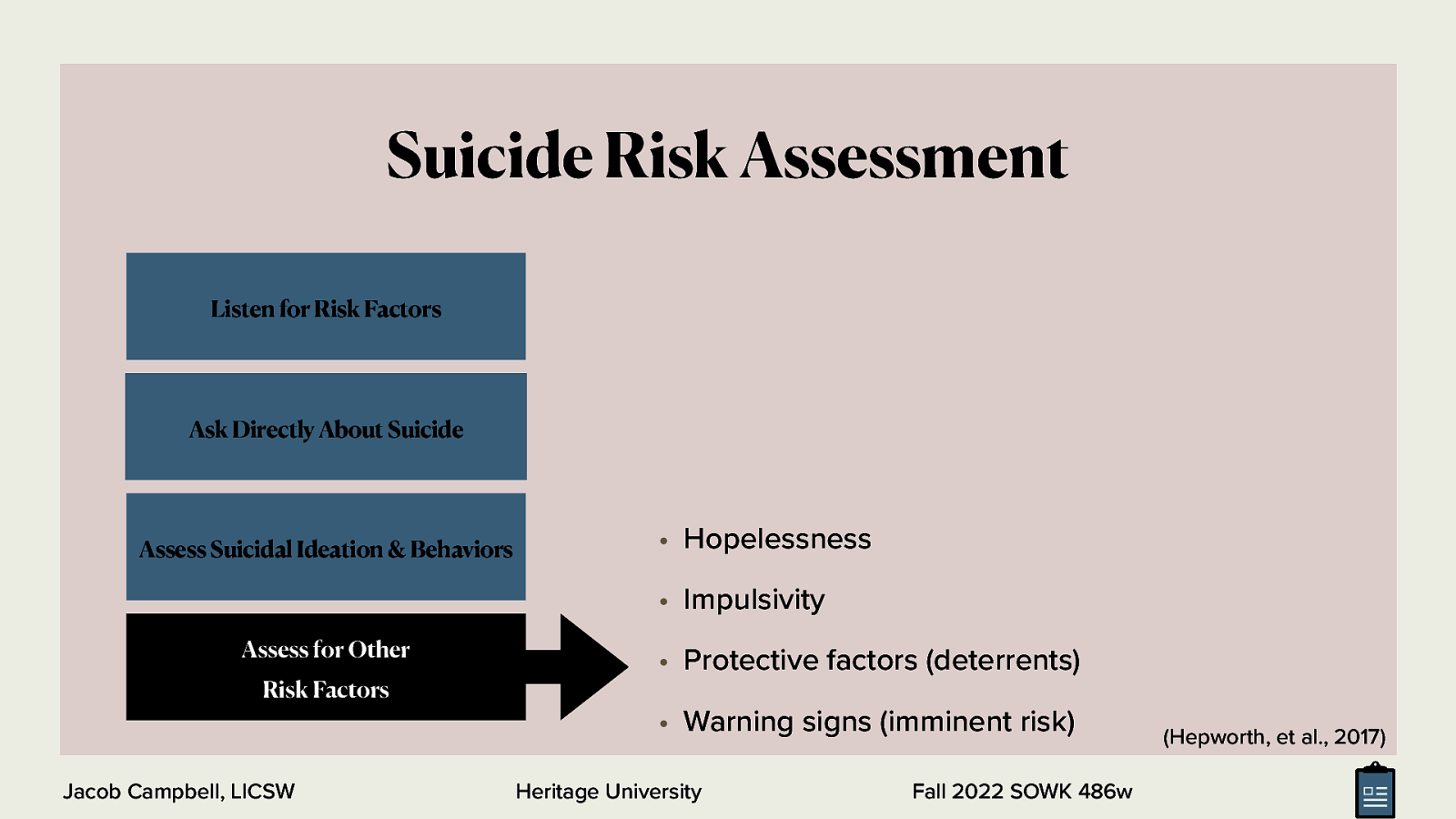
Suicide Risk Assessment Listen for Risk Factors Ask Directly About Suicide Assess Suicidal Ideation & Behaviors • Hopelessness • Impulsivity Assess for Other Risk Factors • Protective factors (deterrents) • Warning signs (imminent risk) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w (Hepworth, et al., 2017)
Elder Assessment Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Adequacy of Client’s Environments • A physical environment that is adequate, is stable, and fosters health and safety (this includes housing as well as surroundings that are free of toxins and other health risks) • Adequate social support systems (e.g., family, relatives, friends, neighbors, organized groups) • A liation with a meaningful and responsive faith community • Access to timely, appropriate, a ordable health care (including vaccinations, physicians, dentists, medications, and nursing homes) • Access to safe, reliable, a ordable child and elder care services • Access to recreational facilities • Transportation—to work, socialize, utilize resources, and exercise rights as a citizen • Adequate housing that provides ample space, sanitation, privacy, and safety from hazards and pollution (both air and noise) • Responsive police and re protection and a reasonable degree of security • Safe and healthful work conditions • Su cient nancial resources to purchase essential resources (e.g., food, clothing, housing) • Adequate nutritional intake • Predictable living arrangements with caring others (especially for children) • Opportunities for education and self-ful llment • Access to legal assistance • Employment opportunities Heritage University fi ff ff fi fi ffi ffi Jacob Campbell, LICSW Fall 2022 SOWK 486w (Hepworth, et al., 2017)
Intrapersonal Functioning Biophysical Functioning • Physical characteristics and • Alcohol use and abuse • Use and abuse of other presentation • Physical health • Use and abuse of medications, • Dual diagnosis: comorbid alcohol, and drugs addictive and mental disorders Cognitive/Perceptual Functioning • Intellectual functioning • Values • Judgment • Misconceptions • Reality testing • Self-concept • Coherence • Assessing thought • Cognitive lexibility f f Jacob Campbell, LICSW Affective Functioning substances • Emotional control • Major depressive • Range of emotions disorder • Appropriateness of • Suicidal risk • Behavioral Functioning affect • Assessing affective disorders • Bipolar disorder • Excesses • Risk of violence • De iciencies • Motivation disorders (Hepworth, et al., 2017) Heritage University Fall 2022 SOWK 486w
Assessing Aggression • Personal history • Interpersonal relationships and social supports • Psychological factors • Physical conditions • History of violence • Current threats and plans of violence • Current crisis and situation (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Assessing Person-In-Environment Fit • Environmental Systems • A rming • Physical environment • Harmful • Adequacy • Spirituality and a liation with a faith community • Health • Spirituality • Safety • Religion • Social support systems • Cognitive, a ective, and behavioral dimensions of faith • Missing (Hepworth, et al., 2017) ffi ff ffi Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Biopsychosocial Assessments • Identifying information (e.g., name, age, referral source, brief overview of the presenting problem) • A history of the present circumstances (i.e., the presenting problem, symptoms) • The past psychiatric and medical history of the client and the client’s family (e.g., injuries, operations, medical conditions, medication, ongoing medical treatment) • The client’s social history (e.g., overview of client’s childhood, family structure, living situation, employment and employment history, educational history, hobbies, daily routine, religious or spiritual preferences, friends, past trauma, substance use) • A mental status exam and DSM-5 diagnosis • A formulation (e.g., a statement that summarizes and synthesizes the most important aspects of the case to create a story of the client and his or her past and presenting problems) • For children and adolescents, a brief overview of developmental milestones may be included, addressing the age at which he/she began crawling, walking, talking, toilet training, and so on. (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w

Common Role and Developmental Transitions for Older Age Group • Work, career choices • Separation or divorce • Health impairment • Institutionalization • Parenthood • Single parenthood • Post-parenthood years • Death of a spouse or partner • Geographic moves and migrations • Military deployments • Marriage or partnership commitment • Retirement (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Common Role and Developmental Transitions for Younger Age Group • Changing grades, especially transitioning to middle school or high school • The birth of a sibling • Illness of a parent or caregiver • Loss of social status at school through bullying or peer victimization • Breaking up with a dating partner • The loss of a friendship either through death or argument • Death of a parent or caregiver • Personal illness • Questions surrounding sexual identity • Addition of a new stepparent to a divorced family (Hepworth, et al., 2017) Jacob Campbell, LICSW Heritage University Fall 2022 SOWK 486w
Typical Wants Involved in Presenting Problems • To have less family con ict • To overcome depression • To feel valued by one’s spouse or partner • To have more friends • To be self-supporting • To be included in decision making • To achieve greater companionship in marriage or relationship • To get discharged from an institution • To gain more self-con dence • To make a di cult decision • To master fear or anxiety • To have more freedom • To cope with children more e ectively • To control one’s temper (Hepworth, et al., 2017) ff Heritage University fl fi ffi Jacob Campbell, LICSW Fall 2022 SOWK 486w

Week nine is a continuation of the work we started in week seven and looking at assessments. The focus is diving more into social histories, with an opportunity to practice asking questions related to this in small groups. As well, students do their teach-back activity if there is time we will do some activities around genograms and eco-maps.
 for free. You
can too.
for free. You
can too.